Blog

For research use only. Material is supplied as a lyophilized reference compound with HPLC purity verification.
- Key Facts at a Glance
- Triple agonist mechanism — why dosing is different
- Published dose-escalation protocol
- TRIUMPH phase 2 and phase 3 dosing schedules
- Alternate conservative schedule
Last updated: 11 May 2026 · Reviewed by the Emirates Peptides Research Team · 12-minute read · 8 sources cited
GLP-3 research protocols are converging on a standard dose-escalation pattern drawn from the Phase 2 obesity and diabetes trials. If you are designing a research study or comparing reported dosing against what appears in forums and case reports, this guide summarises the actual clinical-trial escalation schedule, how researchers reconstitute the lyophilised peptide, the TRIUMPH phase 2 and phase 3 dosing tables published by Eli Lilly, and the side-effect considerations that shape dose-titration decisions.
The figures below are taken from published human clinical trials conducted by Eli Lilly and from peer-reviewed literature. GLP-3 supplied by Emirates Peptides is provided strictly for in-vitro and laboratory research. Dose schedules are referenced so researchers can design studies consistent with published protocols, not as prescriptive human-use guidance.
01 · Mechanism
Triple agonist mechanism — why dosing is different
How GLP-1, GIP, and glucagon receptors interact in a single peptide.

GLP-3 is a single peptide that activates three distinct receptors: GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide), and the glucagon receptor. Each receptor contributes a different metabolic effect — GLP-1 drives insulin release and satiety, GIP modulates fat metabolism, and the glucagon component increases energy expenditure. Because the glucagon agonism is unique among current GLP-1 class peptides, the dosing curve and side-effect profile differ meaningfully from Semaglutide and Tirzepatide. This is why glp-3 research protocols include a longer, more cautious initiation phase: the glucagon component is what drives the larger absolute weight-reduction effect, but it is also the contributor that requires the most careful titration to avoid resting-heart-rate elevation and persistent GI symptoms.
02 · Protocol
Published dose-escalation protocol
Latest research insights. No spam, ever.
The stepwise 24-week schedule used across the Phase 2 TRIUMPH obesity trial.
The Phase 2 TRIUMPH obesity trial (Jastreboff et al., 2023) used a stepwise escalation over 24 weeks, reaching a top dose of 12 mg per week. The pattern looked like this:
| Phase | Weeks | Weekly dose | Purpose |
|---|---|---|---|
| Initiation | 1–4 | 2 mg | Tolerability assessment |
| Titration 1 | 5–8 | 4 mg | Gradual receptor engagement |
| Titration 2 | 9–12 | 6 mg | Mid-range dosing |
| Titration 3 | 13–20 | 8 mg | Approaching steady-state efficacy |
| Maintenance | 21+ | 10–12 mg | Top-dose protocol |
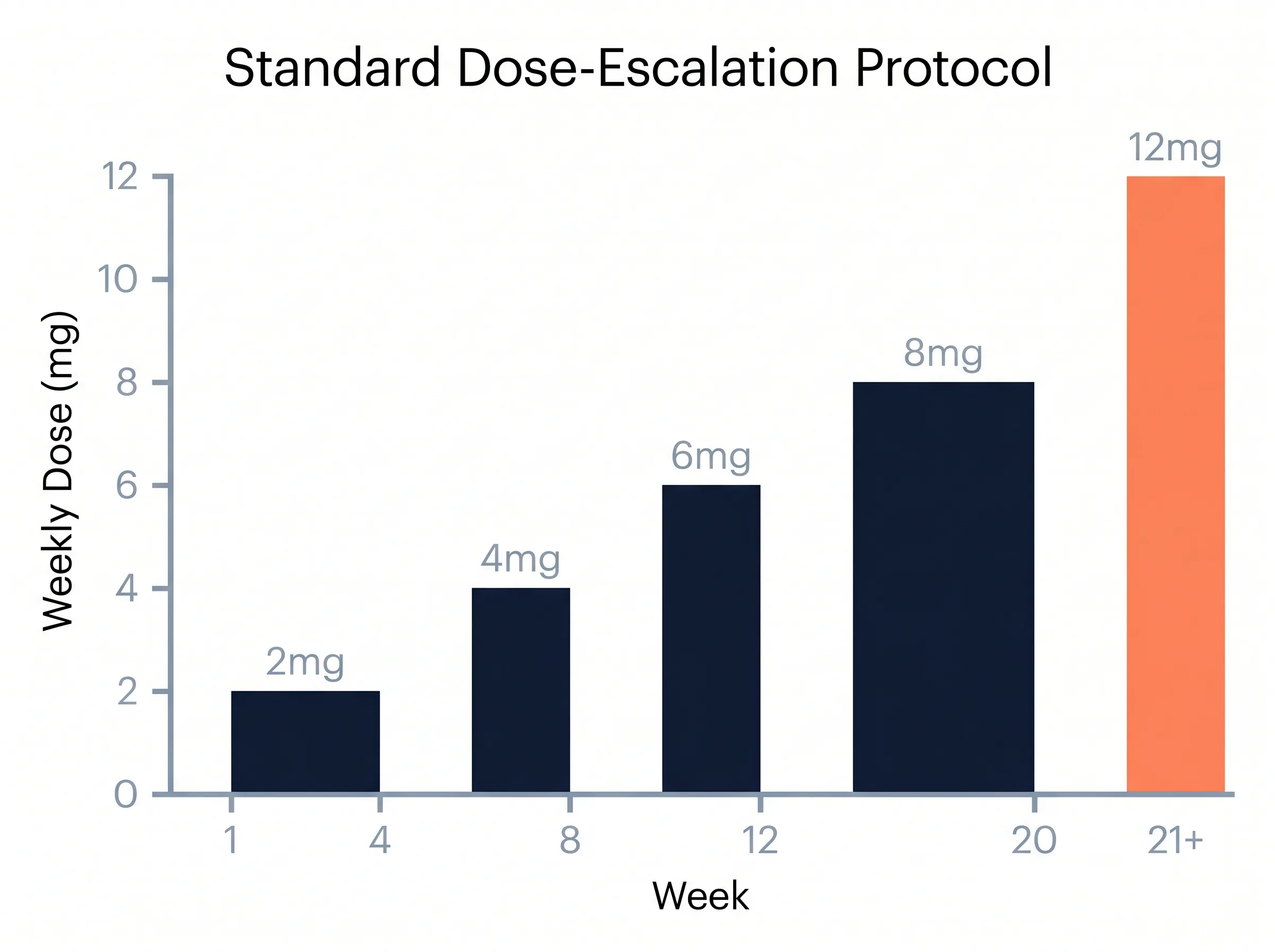
The rationale behind slow escalation is entirely about gastrointestinal tolerability. Nausea, diarrhea, and reduced appetite are the most commonly reported adverse events and cluster heavily in the weeks immediately after each dose increase. Extending each step by 1–2 weeks beyond the protocol minimums often improves subject adherence without diminishing endpoint outcomes.
03 · Trials
TRIUMPH phase 2 and phase 3 dosing schedules
Eli Lilly’s five-trial clinical development plan, dose by dose.

The TRIUMPH programme is Eli Lilly’s clinical development plan for GLP-3. Several published and in-progress trials share a near-identical dosing skeleton, with the main variation being the length of the maintenance phase and the maximum dose tested.
| Trial | Phase | Population | Escalation | Top dose | Duration |
|---|---|---|---|---|---|
| TRIUMPH-1 | Phase 2 | Obesity (BMI ≥ 30) | 2 → 4 → 8 → 12 mg over 24 weeks | 12 mg | 48 weeks |
| TRIUMPH-2 | Phase 2 | Type 2 diabetes | 2 → 4 → 8 → 12 mg over 24 weeks | 12 mg | 36 weeks |
| TRIUMPH-3 | Phase 3 | Obesity + cardiovascular risk | 2 → 4 → 8 → 12 mg over 28 weeks (extended) | 12 mg | 76 weeks |
| TRIUMPH-4 | Phase 3 | Obesity + knee osteoarthritis | 2 → 4 → 8 → 12 mg over 24 weeks | 12 mg | 68 weeks |
| TRIUMPH-5 | Phase 3 | Obesity (long-term safety) | 2 → 4 → 8 → 12 mg over 24 weeks | 12 mg | 156 weeks |
Two practical implications for research design: (1) the dose-escalation skeleton is essentially identical across all phases, which means the Phase 2 schedule above is a defensible reference for any new protocol; (2) the longer maintenance arms in Phase 3 are where most of the weight-reduction endpoint accrues, suggesting research studies should plan for at least 36–48 weeks of total observation if the goal is to capture full effect rather than initiation tolerability alone.
04 · Alternates
Alternate conservative schedule
A slower titration path for subjects sensitive to GI side effects.
Some reported research protocols use a slower escalation for subjects particularly sensitive to GI effects:
2mg/wk
Weeks 1 — 8
Extended initiation
Lowest-dose tolerability assessment. The longest, gentlest phase of this conservative protocol.
4mg/wk
Weeks 9 — 12
Gradual engagement
First true titration step. GI symptoms peak briefly then resolve within ~2 weeks.
6mg/wk
Weeks 13 — 20
Mid-range steady state
Conservative protocols often hold at this dose. Endpoint accrual measurably begins.
8mg/wk
Weeks 21+
Individualised response
Hold at 8 mg or continue titration based on individual tolerability and endpoint goals.
This slower schedule sacrifices peak weight-reduction magnitude for better tolerability — a tradeoff that often makes sense in research protocols where retention rather than maximum endpoint is the priority.
Is bi-weekly (every-2-weeks) dosing viable?
Published protocols all use weekly dosing, but the question comes up often enough in research forums to address directly. With a ~6-day plasma half-life, bi-weekly dosing produces a meaningful trough between doses — concentrations fall to roughly 25–40% of peak at the 14-day mark, depending on the dose. The two practical consequences:
↓AUC
Reduced exposure
Reduced steady-state exposure
Efficacy endpoints are tied to area-under-curve. Bi-weekly schedules likely under-deliver compared to the same nominal dose given weekly.
↕peak
Sharper swing
Sharper peak-trough swing
Each dose lands on a “fresh” receptor state. Bi-weekly can feel worse than weekly even though average exposure is lower.
The pragmatic recommendation in nearly every published protocol remains weekly dosing. If a research subject genuinely cannot tolerate weekly steps, the better answer is usually to extend each dose step (e.g. 8 weeks at 2 mg instead of 4 weeks) rather than to space doses further apart.
05 · Reconstitution
Reconstitution math
BAC water volumes, concentrations, and unit-syringe math for 10, 20, and 30 mg vials.

GLP-3 ships as a lyophilised powder. Emirates Peptides offers 10 mg, 20 mg, and 30 mg vial sizes. Each vial is reconstituted with bacteriostatic water (not saline, not tap water, not sterile water for injection) before drawing research doses.
The following concentrations are commonly chosen because they make dose math convenient on an insulin syringe:
| Vial size | BAC water added | Final concentration | Weekly dose examples |
|---|---|---|---|
| 10 mg | 2 mL | 5 mg/mL | 2 mg = 0.4 mL · 4 mg = 0.8 mL |
| 20 mg | 2 mL | 10 mg/mL | 4 mg = 0.4 mL · 8 mg = 0.8 mL |
| 30 mg | 3 mL | 10 mg/mL | 6 mg = 0.6 mL · 12 mg = 1.2 mL |

A few practical notes on the math: the 30 mg vial with 3 mL bacteriostatic water produces a 10 mg/mL concentration, which is the most flexible choice for high-end protocols because a 12 mg weekly dose lands at a clean 1.2 mL draw. If you only need lower doses (2–4 mg weekly), reconstituting a 10 mg vial with 2 mL of BAC water gives a 5 mg/mL concentration, which spreads the dose across more syringe graduations and improves draw accuracy at the small end.
Don’t draw the BAC water aggressively and squirt it directly onto the lyophilised cake. Aim the stream against the glass wall of the vial, swirl gently after addition (do not shake), and wait 1–3 minutes for full dissolution. The reconstituted solution should be clear and colourless; any haze, particulates, or yellow tint indicates a degradation problem and the vial should not be used.
Post-reconstitution stability and storage

Storage rules for the reconstituted solution are simple and worth following closely because the peptide is sensitive to temperature swings and light:
2–8°C
28-day window
Refrigerated, protected from light
Full potency preserved for approximately 28 days from reconstitution.
≤25°C
Counts vs 28 days
Room temperature
Acceptable for short periods (travel), but cumulative time at room temperature counts against the 28-day window.
✕freeze
Repeated cycles
Do not freeze
Repeated freeze-thaw cycles fragment the peptide. A reconstituted vial that has been frozen should be discarded.
✓check
Visual inspection
Inspect before every draw
Clear and colourless = usable. Cloudy, hazy, particulate, or yellow-tinted = discard.
If a vial reaches 28 days post-reconstitution with material remaining, the conservative research-protocol position is to discard the remainder and start a fresh vial, even if the solution still looks visually fine. Some labs extend to 35 days based on stability data from analogous GLP-1 peptides, but published TRIUMPH protocols use the 28-day boundary.
Reconstituting a 30 mg vial with exactly 3 mL of bacteriostatic water produces a clean 10 mg/mL concentration — so a 12 mg weekly dose lands at a precise 1.2 mL syringe draw without any mental math during a research session.
06 · Injection
Injection site and timing
Where to inject, how often, and how to rotate sites across weeks.
Research protocols typically specify subcutaneous injection with a standard insulin syringe. Common sites are the abdomen (approximately 2 cm away from the navel), outer thigh, or upper arm. Rotating sites between weekly injections reduces lipohypertrophy risk — a practical consideration drawn from diabetes research rather than a GLP-3-specific finding.

The 6-day half-life allows flexible weekly scheduling. Most reported protocols use the same day each week (Monday morning or Sunday evening are common) to maintain steady circulating concentrations. A missed dose up to 2 days late is typically administered as planned, and the next dose stays on the regular weekly schedule. Missed doses beyond 3 days generally return to the next scheduled week.

Syringe selection — 29G vs 31G
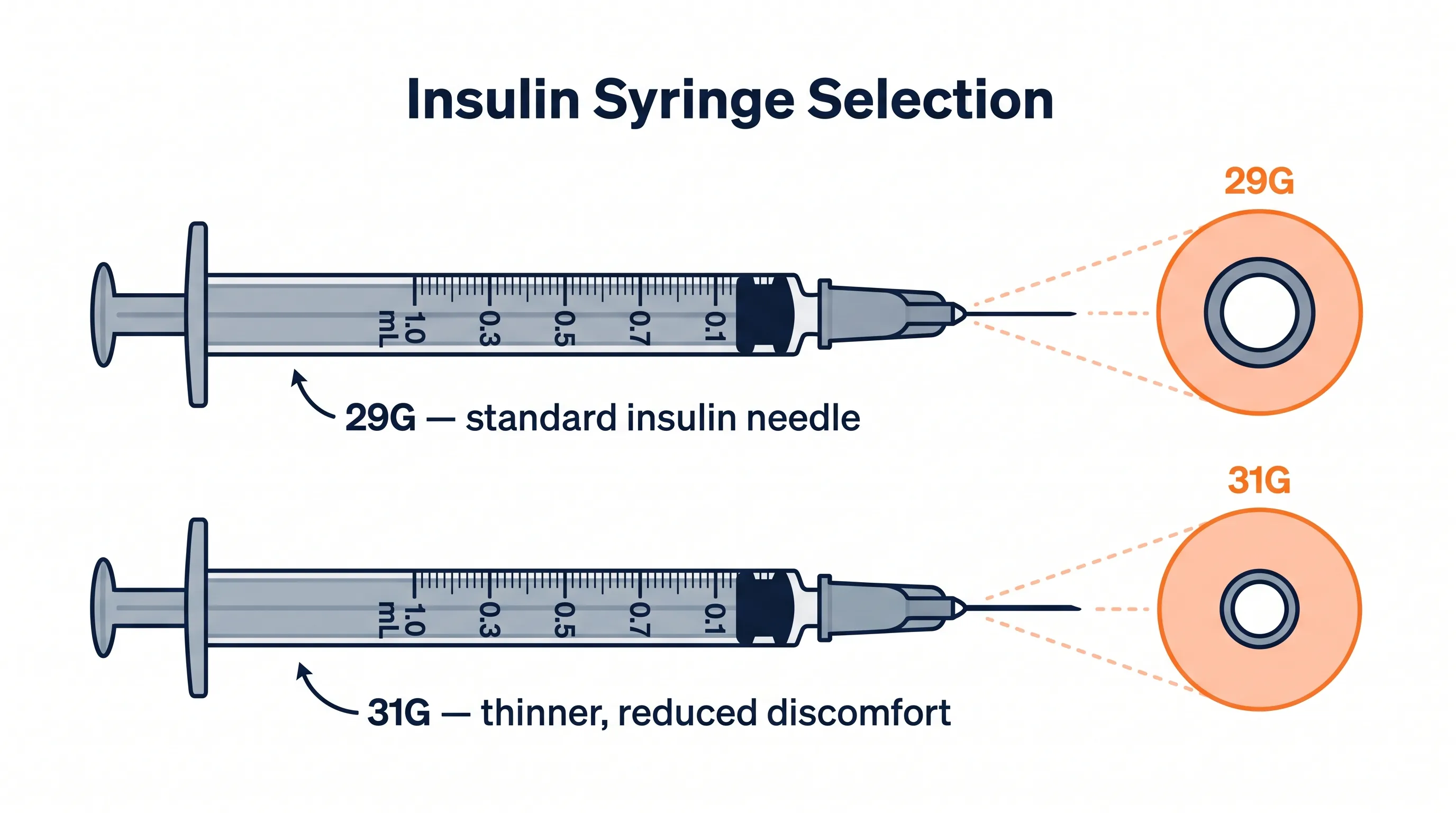
Almost all reported research protocols use 1 mL insulin syringes with a 5/16-inch (8 mm) needle. The two common needle gauges are 29G and 31G — both are appropriate, with the choice usually driven by subject preference:
29G
Thicker needle
Faster draw, larger volumes
Slightly thicker needle, faster draw from the vial. Preferred when reconstituted solution is more viscous or the dose volume exceeds 1 mL.
31G
Thinner needle
Lower discomfort, smaller doses
Thinner needle, less discomfort on injection. Ideal for the small subcutaneous doses (0.1–0.5 mL) typical of mid-titration weeks.
The graduations on a 1 mL insulin syringe are typically in 0.02 mL increments (sometimes labelled in insulin units: 100 units = 1 mL). This is the practical reason for choosing reconstitution concentrations of 5 or 10 mg/mL — both produce dose volumes that land cleanly on visible graduations rather than between them.
07 · Side effects
Side-effect considerations that shape dosing decisions
When to hold, step back, or push forward — guided by GI tolerability.
The decision to hold, step back, or advance a dose is dominated by GI tolerability. Published protocols and research case reports converge on the following rules of thumb:
01level
No dose change
Mild nausea
No dose change. Usually resolves within 3–7 days of a new step.
02level
Extend step
Moderate nausea / occasional vomiting
Extend the current step by 2–4 weeks before the next increase.
03level
Step down
Severe or persistent vomiting
Step down to the previous tolerated dose; reassess before any further increases.
♥HR
> 15 bpm rise
Resting heart-rate elevation
Evaluate as part of the glucagon-receptor mechanism. Typically attenuates over 4–8 weeks; consider holding if persistent.

The shape of the side-effect curve above is consistent across the published TRIUMPH-1 and TRIUMPH-2 data: GI symptoms cluster sharply in the first week after each escalation, decline through week 2, and largely resolve by the end of week 4. This is the empirical basis for the 4-week step-length in the standard protocol — it gives the receptor population time to adapt before the next increase. Cutting steps shorter (e.g. 2 weeks per step) increases dropout dramatically without faster endpoint accrual.
TRIUMPH-1 (NEJM 2023) reported resting-heart-rate elevation of 6–8 bpm on average at the 12 mg arm, typically attenuating after the maintenance phase began. Researchers designing studies should plan for cardiovascular monitoring through the first 12–16 weeks of the protocol.
These are observations drawn from the published literature, not prescriptive rules. Individual research subjects vary considerably; protocol design and adjustment are the responsibility of the qualified research professional.
08 · Comparison
How dosing compares to other GLP-1-class peptides
GLP-3 against Semaglutide and Tirzepatide, side by side.

2.4mg/wk
16-week ramp
Semaglutide (Ozempic / Wegovy)
0.25 mg → 2.4 mg weekly escalation. Much smaller absolute dose range reflects Semaglutide’s different pharmacokinetics.
15mg/wk
20-week ramp
Tirzepatide (Mounjaro / Zepbound)
2.5 mg → 15 mg weekly. Close to GLP-3’s range but without the glucagon-receptor component.
12mg/wk
20–24 week ramp
GLP-3 (research)
2 mg → 12 mg weekly. Similar escalation length to Tirzepatide, with the unique triple-agonist mechanism.
For a deeper comparison of mechanism, efficacy, and side-effect profile, see GLP-3 vs Tirzepatide vs Semaglutide.
09 · FAQ
Frequently asked questions
Quick answers to the most common research-protocol questions.
What is the maximum GLP-3 dose in the research literature?
Phase 2 obesity trials went up to 12 mg weekly. Phase 3 trials in progress as of May 2026 are examining doses in this range. Higher doses have not been tested in published human research.
How long does it take to reach full effect?
Peak weight-reduction is typically observed between weeks 36 and 48 of continuous weekly dosing at the top protocol dose. Early changes in appetite and satiety appear within the first 2–4 weeks of initiation dose.
Can GLP-3 be injected every 2 weeks instead of weekly?
Published protocols all use weekly dosing. The 6-day half-life means that biweekly dosing would produce significant trough concentrations that could reduce efficacy and worsen side effects when the next dose is administered. Weekly dosing remains standard.
What syringe size is appropriate for GLP-3 research dosing?
Standard insulin syringes (1 mL, 29–31 gauge, 5/16″ needle) are suitable for subcutaneous administration of GLP-3 at all concentrations described above. 29G gives faster draw; 31G is slightly more comfortable.
How should GLP-3 be stored after reconstitution?
Refrigerated (2–8 °C), protected from light, and used within 28 days. Do not freeze reconstituted solutions; repeated freeze-thaw cycles destroy the peptide.
Is a 15 mg weekly GLP-3 dose ever used?
15 mg has not been tested in published human GLP-3 trials. The TRIUMPH programme caps at 12 mg per week. Anecdotal forum reports of 15 mg dosing are not supported by clinical evidence and exceed the maximum tested research range.
What if a research subject misses a GLP-3 dose by more than 3 days?
Published protocols generally have the subject skip the missed dose and resume at the next scheduled weekly injection. Doubling-up to “catch up” is not recommended — peak concentrations after a double dose can exacerbate GI symptoms substantially.
Is monthly (every-4-weeks) GLP-3 dosing possible?
No. The 6-day half-life makes monthly dosing pharmacologically impractical — trough concentrations 28 days after a dose are negligible. No published protocol uses monthly dosing.
What happens at the maximum 12 mg GLP-3 dose in trials?
TRIUMPH-1 reported mean weight reduction of approximately 24% from baseline at the 12 mg arm by week 48, with the most common adverse events being mild-to-moderate nausea, diarrhea, and vomiting concentrated in the escalation phase. Resting heart rate elevation of 6–8 bpm on average was observed, typically attenuating after the maintenance phase began.
Why use bacteriostatic water and not regular sterile water for GLP-3 reconstitution?
Bacteriostatic water contains 0.9% benzyl alcohol, which prevents microbial growth in the reconstituted vial across the 28-day use window. Regular sterile water has no preservative and reconstituted vials must be used within hours instead of weeks. Saline is also unsuitable because the salt content can affect peptide stability.
10 · References
References and clinical-trial sources
Peer-reviewed papers and ClinicalTrials.gov entries cited throughout.
For research-protocol design, the following sources are the primary references for the schedules above:
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist GLP-3 for Obesity — A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514–526. (TRIUMPH-1 obesity)
- Rosenstock J, Frias J, et al. GLP-3, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial. The Lancet. 2023;402(10401):529–544. (TRIUMPH-2 diabetes)
- ClinicalTrials.gov registrations: NCT04881760 (TRIUMPH-1), NCT04867785 (TRIUMPH-2), NCT05882045 (TRIUMPH-3), NCT05125731 (TRIUMPH-4), NCT05929066 (TRIUMPH-5).
- Coskun T, Urva S, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept. Cell Metabolism. 2022;34(9):1234–1247.
Related reading
- GLP-3 UAE: Complete Research Peptide Guide
- What is GLP-3? Plain-language explainer
- GLP-3 vs Tirzepatide vs Semaglutide
- GLP-3 product page
Disclaimer: All figures are from published research protocols. GLP-3 supplied by Emirates Peptides is for laboratory and in-vitro research use only. Not for human administration.
Was this article helpful?
🔬 Related Research Peptides



Explore Research-Grade Peptides
HPLC-verified, lab-tested peptides for your scientific research. Fast delivery across the UAE.
Browse All PeptidesRelated Articles


Selected Research References
Selected scientific references for research context only. Products remain for laboratory research use and are not for human use.
- Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial
- Tirzepatide Once Weekly for the Treatment of Obesity
- Tirzepatide as Compared with Semaglutide for the Treatment of Obesity
- Once-Weekly Semaglutide in Adults with Overweight or Obesity
- Once-weekly cagrilintide for weight management in people with overweight and obesity
Emirates Peptides Research Team
A dedicated coalition of biochemists and clinical researchers focusing on advanced peptide synthesis and pharmacological applications. All data is verified against current clinical trials.
